


Usually above 3,000m (9,800 ft)
Usually above 4,000m (13,100 ft)
Can kill within 12-24 hours untreated
Can lead to coma/death within 24-72 hours
Immediate descent 500-1,000m
Nifedipine 20mg slow-release
Dexamethasone 8mg initial dose
Pheriche (4,371m) & Manang (3,540m)
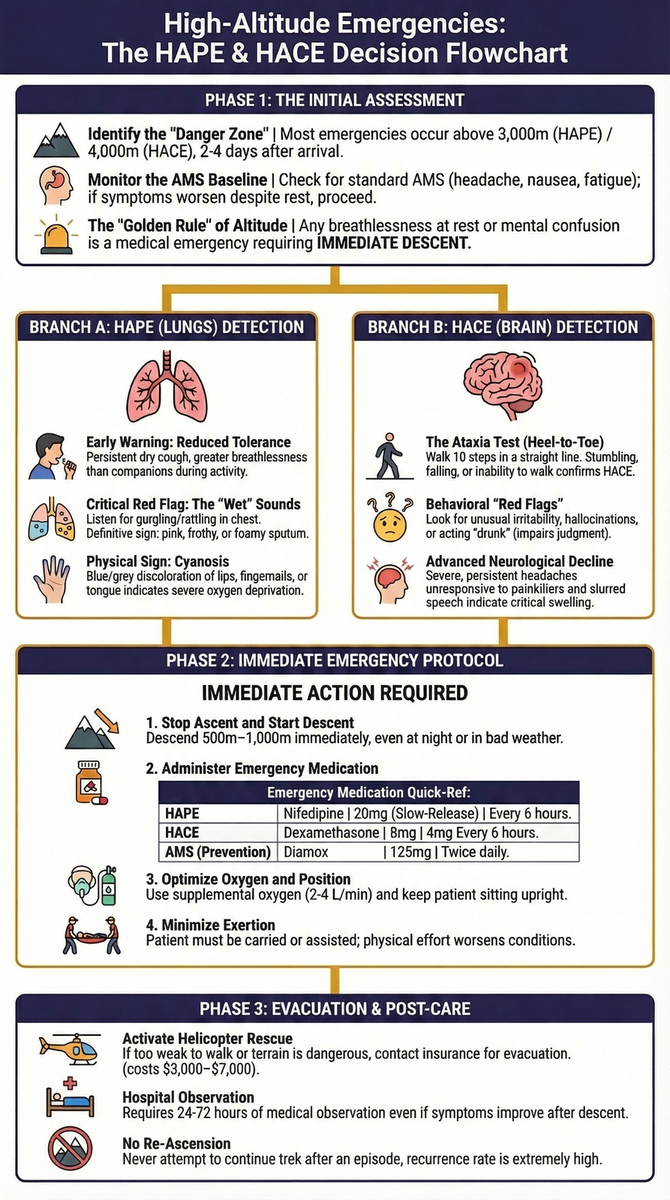
HAPE and HACE: The Altitude Emergencies Every Nepal Trekker Must Know
HAPE and HACE are the two life-threatening forms of altitude sickness in Nepal: HAPE is fluid in the lungs (breathlessness, cough), HACE is fluid in the brain (confusion, loss of coordination). Both demand immediate descent of 500-1,000m. Medications buy time, but descent is the only cure.
High Altitude Pulmonary Edema (HAPE) and High Altitude Cerebral Edema (HACE) are the two most dangerous altitude-related medical emergencies that trekkers face in Nepal. Every year, trekkers on popular routes like Everest Base Camp, the Annapurna Circuit, and the Manaslu Circuit develop these life-threatening conditions. Some are evacuated by helicopter. Some descend on foot with the help of their guides. And tragically, a few do not survive.
What makes HAPE and HACE so dangerous is not their rarity -- it is the speed at which they can progress from manageable symptoms to fatal outcomes, and the tendency for trekkers to dismiss early warning signs as "normal" altitude discomfort. Understanding the difference between ordinary altitude sickness and a genuine medical emergency can mean the difference between a successful trek and a tragedy.
This guide is specifically focused on HAPE and HACE -- the severe, life-threatening end of the altitude illness spectrum. It covers how to recognize early symptoms, what to do in an emergency, how these conditions differ from standard Acute Mountain Sickness (AMS), and the medications and evacuation options available on Nepal's trekking routes.
Critical Medical Disclaimer: Life-Threatening Conditions
HAPE and HACE are medical emergencies that can be fatal within hours. If you suspect either condition, begin descent immediately. Do not wait until morning. Do not wait for symptoms to "improve." Do not attempt to treat these conditions at altitude without descending. This guide provides educational information to help you recognize and respond to these emergencies, but it does not replace professional medical training or care. Always consult a physician experienced in altitude medicine before trekking above 3,000m. In an emergency, descend first and seek medical help as soon as possible.
Understanding the Altitude Illness Spectrum: How AMS Becomes Deadly
Altitude illness is not a binary condition -- you do not simply "have it" or "not have it." Instead, it exists on a spectrum of severity, and HAPE and HACE represent the most dangerous end of that spectrum.
The Progression from AMS to HACE
Acute Mountain Sickness (AMS) is the most common form of altitude illness, affecting 50-85% of trekkers who ascend above 4,500m. Its symptoms -- headache, nausea, fatigue, poor appetite, and difficulty sleeping -- are uncomfortable but not immediately dangerous. For most trekkers, AMS resolves with rest, hydration, and proper acclimatization.
However, if AMS symptoms are ignored and a trekker continues ascending, AMS can progress to High Altitude Cerebral Edema (HACE). The transition is not always gradual. Some trekkers go from "feeling a bit rough" to confused and unable to walk in a matter of hours.
The AMS-to-HACE progression typically follows this pattern:
- Mild AMS -- Headache, fatigue, mild nausea (manageable, monitor closely)
- Moderate AMS -- Persistent headache unresponsive to painkillers, vomiting, significant fatigue
- Severe AMS -- Intense headache, repeated vomiting, extreme fatigue, early confusion
- HACE -- Confusion, ataxia (loss of coordination), altered consciousness, potential coma
The Progression from AMS to HAPE
HAPE can develop alongside AMS, but it can also appear independently. Some trekkers develop HAPE without ever experiencing classic AMS symptoms, which makes it particularly treacherous. HAPE involves fluid accumulating in the lungs, reducing the body's ability to oxygenate blood.
The HAPE progression:
- Reduced exercise tolerance -- Getting more breathless than companions at the same altitude
- Dry cough -- Persistent, worsening cough, especially at rest or lying down
- Breathlessness at rest -- Difficulty breathing even when sitting still
- Wet cough with frothy/pink sputum -- Fluid in the lungs produces audible gurgling
- Severe HAPE -- Cyanosis (blue lips/fingertips), inability to walk, drowning sensation
Pro Tip
HAPE: High Altitude Pulmonary Edema
What HAPE Is
High Altitude Pulmonary Edema is a condition in which fluid leaks from blood vessels into the air sacs (alveoli) of the lungs. As fluid accumulates, the lungs become progressively less able to transfer oxygen into the bloodstream. In essence, the trekker begins to drown in their own body fluid at altitude.
HAPE is caused by exaggerated pulmonary hypertension -- when the blood vessels in the lungs constrict unevenly in response to low oxygen levels at altitude, causing fluid to be forced through vessel walls and into lung tissue.
Who Is at Risk
HAPE can strike anyone regardless of age, fitness level, or previous high-altitude experience. However, certain factors increase risk:
- Rapid ascent -- Gaining more than 500m of sleeping altitude per day above 3,000m
- Previous HAPE episode -- Individuals who have had HAPE before have a 60% recurrence rate
- Respiratory infections -- Even mild colds can increase susceptibility
- Heavy exertion at altitude -- Pushing too hard on arrival at a new elevation
- Cold temperatures -- Cold air increases pulmonary artery pressure
- Individual susceptibility -- Some people are genetically predisposed to exaggerated pulmonary vasoconstriction
- Older age -- Trekkers over 65 have shown roughly a 3-fold higher risk of HAPE (no equivalent increase was found for AMS or HACE)
- Altitude reached -- Risk increases significantly above 3,000m, though cases have been reported as low as 2,500m
Fitness Does Not Protect You
One of the most dangerous myths in trekking is that physically fit individuals are immune to altitude illness. In reality, HAPE has killed elite athletes, marathon runners, and experienced mountaineers. Fitness has no correlation with altitude susceptibility. In fact, fit individuals may be at higher risk because they tend to push harder and ascend faster, ignoring early symptoms as mere fatigue.
When HAPE Develops
HAPE typically develops 2-4 days after arrival at altitude, most commonly during the second or third night at a new elevation. Symptoms often worsen at night when the body is horizontal and fluid redistribution increases. This is why many HAPE cases are discovered in the morning when a trekker wakes up severely breathless -- or is found unresponsive by their trekking companions.
On Nepal's popular routes:
- Everest Base Camp route: Risk is highest between Namche Bazaar (3,440m) and Lobuche (4,940m), particularly if trekkers skip acclimatization days
- Annapurna Circuit: Risk peaks around Manang (3,540m) to Thorong La High Camp (4,925m)
- Manaslu Circuit: Risk increases from Samagaun (3,530m) through Larkya La (5,160m)
Early Symptoms of HAPE
Recognizing HAPE early is critical because it is far easier to treat in its initial stages:
- Dry, persistent cough -- Initially non-productive, worsening over hours
- Breathlessness with minimal exertion -- More than expected for the altitude and activity level
- Reduced exercise tolerance -- Significantly slower than usual or slower than companions
- Fatigue beyond what is normal -- Disproportionate exhaustion for the day's effort
- Mild chest tightness -- A feeling of constriction or heaviness in the chest
- Elevated resting heart rate -- Heart rate 20+ beats per minute above your normal resting rate
- Difficulty sleeping due to breathlessness -- Needing to sit up to breathe
Advanced Symptoms of HAPE
When HAPE has progressed to a dangerous stage, the following symptoms appear:
- Gurgling or rattling sounds when breathing -- Audible without a stethoscope, sometimes described as "bubbling"
- Pink or frothy sputum -- Coughing produces foamy, blood-tinged fluid (this is a definitive sign)
- Severe breathlessness at rest -- Cannot speak in full sentences, struggling to breathe even while sitting still
- Cyanosis -- Blue or grey discoloration of lips, fingernails, or tongue due to oxygen deprivation
- Rapid, shallow breathing -- Respiratory rate above 25-30 breaths per minute at rest
- Confusion or drowsiness -- Brain is not receiving enough oxygen (may indicate concurrent HACE)
- Inability to walk or stand -- Too breathless and weak to be mobile
Critical fact: Untreated HAPE can kill within 12-24 hours. Once pink frothy sputum appears, the condition is immediately life-threatening.
HAPE Emergency Response Protocol
If you suspect HAPE in yourself or a fellow trekker, follow this step-by-step protocol:
Step 1: Stop all ascent immediately. Do not go even one meter higher.
Step 2: Begin descent immediately. Descend at least 500-1,000m in elevation. Do not wait until morning. Do not wait to "see if it gets better." HAPE gets worse at the same altitude -- it does not resolve without descent.
Step 3: Minimize exertion during descent. The affected person should be carried or assisted if possible. Physical exertion worsens HAPE. If porters, horses, or yaks are available, use them.
Step 4: Administer supplemental oxygen if available. Flow rate of 2-4 liters per minute. Available at HRA clinics in Pheriche and Manang, and at some larger lodges on popular routes.
Step 5: Administer Nifedipine if available. 20mg slow-release, every 6 hours. Nifedipine reduces pulmonary artery pressure. This medication buys time for descent but does NOT cure the condition.
Step 6: Keep the person sitting upright. A semi-reclined or sitting position reduces fluid accumulation in the lungs compared to lying flat.
Step 7: Evacuate to lower altitude and medical care. If descent on foot is not possible (nighttime on dangerous trail, weather, patient too weak), activate helicopter rescue. Ensure your travel insurance covers emergency evacuation.
Step 8: Do not re-ascend. Even if the person feels better after descending, they should not re-ascend on the same trek. HAPE has a very high recurrence rate.
Recovery from HAPE
The good news about HAPE is that recovery with descent is usually rapid and dramatic. Many trekkers who are severely ill at 4,500m feel significantly better after descending to 3,000m. The lungs begin to clear within hours of reaching lower altitude.
However, medical observation is important even after apparent recovery:
- Observation at a lower-altitude medical facility for at least 24 hours
- Chest X-ray if available to confirm fluid has cleared
- Monitoring of oxygen saturation levels
- Antibiotics may be prescribed if secondary pneumonia is suspected
- Full recovery typically takes 2-5 days at lower altitude
HACE: High Altitude Cerebral Edema
What HACE Is
High Altitude Cerebral Edema is swelling of the brain caused by fluid leakage from blood vessels into brain tissue at altitude. As the brain swells inside the rigid skull, intracranial pressure increases, leading to progressive neurological deterioration. Without treatment, the swelling compresses vital brain structures and causes death.
HACE is the most immediately dangerous form of altitude illness. While HAPE kills by suffocation, HACE kills by brain herniation -- the brain is squeezed downward through the opening at the base of the skull.
Who Is at Risk
HACE typically occurs at altitudes above 4,000m, though rare cases have been documented as low as 3,000m. Risk factors include:
- Rapid ascent -- The primary risk factor
- Previous HACE episode -- Recurrence risk is significant
- Ignoring AMS symptoms -- Most HACE cases develop from untreated AMS
- Dehydration -- Exacerbates the effects of altitude on the brain
- Sleep medications -- Sleeping pills can mask early symptoms and depress breathing
- Individual susceptibility -- Some people are more vulnerable than others, with no reliable way to predict who
When HACE Develops
HACE can develop in two ways:
-
Progressive onset from AMS: Over 12-72 hours, AMS symptoms gradually worsen into HACE. This is the more common pattern and is often recognizable if companions are attentive.
-
Rapid onset: In rare cases, HACE can appear with alarming speed -- a trekker may seem fine at dinner and be confused and unable to walk by morning. This pattern is more common above 5,000m.
On Nepal's routes, HACE is most common:
- Above Gorak Shep (5,164m) on the EBC trek
- Near Thorong La Pass (5,416m) on the Annapurna Circuit
- Near Larkya La Pass (5,160m) on the Manaslu Circuit
- During peak climbing on routes like Island Peak (6,189m) or Mera Peak (6,476m)
Early Symptoms of HACE
- Severe, persistent headache -- Does not respond to standard painkillers (paracetamol/ibuprofen), unlike AMS headache which usually improves
- Confusion or disorientation -- Asking strange questions, not knowing where they are, unable to process simple instructions
- Unusual irritability or behavior changes -- Becoming uncharacteristically aggressive, apathetic, or emotional
- Loss of coordination (ataxia) -- Stumbling, difficulty walking in a straight line, trouble with fine motor tasks like zipping a jacket
- Severe lethargy -- Beyond normal tiredness; reluctance or inability to get out of bed, eat, or drink
- Visual disturbances -- Blurred vision, double vision, seeing halos around lights
- Hallucinations -- Seeing or hearing things that are not there
The Ataxia Test: Your Most Important Tool
The heel-to-toe walking test (also called the tandem gait test) is the single most reliable field test for detecting HACE. It works because the cerebellum -- the brain region controlling coordination -- is particularly vulnerable to altitude-induced swelling.
How to perform the test:
- Draw a straight line on the ground (or find a straight crack, plank, or edge)
- Ask the person to walk along the line, placing one foot directly in front of the other (heel touching toe)
- They should walk at least 10 steps with arms at their sides (not extended for balance)
Interpreting results:
- Normal: Can walk the line without significant wobbling or stepping off
- Concerning: Stumbles, needs to extend arms for balance, steps off the line once or twice
- HACE indicator: Cannot walk the line at all, stumbles repeatedly, needs to grab support, falls
The Ataxia Test Rule
If a trekker with headache and/or AMS symptoms cannot walk a straight line heel-to-toe, assume HACE until proven otherwise and begin immediate descent. Do not wait for additional symptoms. Do not rationalize the result ("they are just tired"). This test has saved lives on Nepal's trails.
Pro Tip
Advanced Symptoms of HACE
If HACE progresses beyond the early stage, the following symptoms indicate a critical emergency:
- Inability to walk without support -- Cannot stand or walk independently
- Slurred speech -- Similar to severe alcohol intoxication
- Incontinence -- Loss of bladder or bowel control
- Persistent vomiting -- Projectile vomiting indicating increased intracranial pressure
- Seizures -- Involuntary convulsions
- Progressive loss of consciousness -- From drowsiness to stupor to coma
- Abnormal pupil response -- One pupil larger than the other (critical sign of brain herniation)
Critical fact: Untreated HACE leads to coma and death within 24-72 hours. Once a person becomes unconscious from HACE, survival without immediate evacuation and intensive medical care is extremely unlikely.
HACE Emergency Response Protocol
Step 1: DESCEND IMMEDIATELY. This is non-negotiable. Even if it is dark, even if the trail is difficult, even if the weather is bad. HACE gets worse with every hour at the same altitude. Descend at least 500-1,000m.
Step 2: Administer Dexamethasone if available. Initial dose of 8mg (oral, intramuscular, or intravenous), followed by 4mg every 6 hours. Dexamethasone is a potent corticosteroid that reduces brain swelling. It buys time for descent, but it does NOT cure HACE.
Step 3: Administer supplemental oxygen if available. 2-4 liters per minute. Helps reduce cerebral vasodilation and swelling.
Step 4: Protect the patient. A confused or ataxic person may injure themselves. Assist them during descent. If they cannot walk, they must be carried.
Step 5: Do not let the person sleep unmonitored. Check on them every 30 minutes during descent. If they lose consciousness, place them in the recovery position (on their side) to prevent choking on vomit.
Step 6: Evacuate. Activate helicopter rescue if descent on foot is impossible or too slow. Every hour matters with HACE.
Step 7: Hospital care. Even after successful descent and apparent improvement, the person needs hospital evaluation. Brain imaging (CT or MRI) may be necessary to rule out other conditions and assess for lasting damage.
When to Descend: The Non-Negotiable Red Flags
When you are unsure whether symptoms are "just AMS" or a genuine emergency, the safest decision is almost always the same one: go down. Descend immediately, at any time of day or night, if any of these appear:
- Confusion or abnormal behavior -- the person is not thinking clearly or is acting out of character
- Loss of coordination -- they fail the heel-to-toe ataxia test or cannot walk a straight line
- Breathlessness at rest -- struggling to breathe while sitting still, not just when exerting
- A cough that is rapidly worsening, especially with frothy or pink sputum
- Symptoms that keep getting worse at the same altitude despite stopping the ascent
A descent of even 300-600m can produce dramatic improvement, and 500-1,000m is the target for a confirmed HAPE or HACE emergency. These are descend-now signs, not wait-and-see signs. Do not let darkness, weather, fatigue, or a fixed itinerary delay the decision -- the cost of descending unnecessarily is a lost day, while the cost of staying too high can be a life. For the full framework on stopping points, see our guide to altitude sickness signs and turnaround rules.
HAPE vs. HACE: How to Tell Them Apart
Distinguishing between HAPE and HACE in the field matters because the specific medications differ, though the primary treatment -- descent -- is the same for both.
| Feature | HAPE | HACE |
|---|---|---|
| Primary organ affected | Lungs | Brain |
| Main early symptom | Breathlessness and cough | Confusion and loss of coordination |
| Typical onset altitude | Above 3,000m | Above 4,000m |
| Onset timing | 2-4 days at altitude, often overnight | Hours to days after AMS onset |
| Key diagnostic sign | Gurgling breath / pink frothy sputum | Failed ataxia test (heel-to-toe walk) |
| Breathing | Rapid, labored, wet sounds | May be normal initially |
| Mental status | Clear initially, confusion late (from hypoxia) | Confusion is an early sign |
| Coordination | May be normal initially | Impaired early |
| Skin color | Cyanosis (blue lips/nails) | May appear normal initially |
| Heart rate | Elevated, rapid | May be normal or elevated |
| Cough | Prominent, productive (frothy/pink) | Absent or mild |
| Primary medication | Nifedipine (20mg slow-release) | Dexamethasone (8mg initial) |
| Speed of death if untreated | 12-24 hours | 24-72 hours |
Can You Have Both HAPE and HACE Simultaneously?
Yes, and it is the most dangerous scenario a trekker can face. HAPE and HACE can develop simultaneously or sequentially, and having one condition increases the risk of developing the other.
Why they occur together:
- HAPE reduces blood oxygen levels, which can trigger or worsen brain swelling (HACE)
- HACE impairs judgment and coordination, making it harder for the person to recognize HAPE symptoms or cooperate with descent
- Both conditions share the same underlying trigger: inadequate acclimatization at altitude
When both conditions are present:
- Administer both Nifedipine (for HAPE) and Dexamethasone (for HACE)
- Supplemental oxygen is critical
- Descent is even more urgent
- The person is unlikely to be able to walk and will need to be carried
- Helicopter evacuation should be the first option, not the last resort
Combined HAPE/HACE Is a Maximum Emergency
If a trekker shows signs of both HAPE (breathlessness, cough, gurgling) and HACE (confusion, ataxia), this is the most dangerous altitude emergency possible. Activate helicopter rescue immediately while beginning assisted descent. Do not wait for conditions to change. Mortality in combined HAPE/HACE without rapid descent and medical intervention is extremely high.
How HAPE and HACE Differ from Normal AMS
Many trekkers experience AMS and naturally wonder whether their symptoms might be something more serious. Understanding the severity boundaries helps you know when to rest and when to run (descend).
| Severity Level | Symptoms | Action Required |
|---|---|---|
| Mild AMS | Headache, mild nausea, fatigue, poor appetite, difficulty sleeping | Rest at current altitude, hydrate, take paracetamol. Do not ascend until symptoms resolve. |
| Moderate AMS | Persistent headache despite medication, vomiting, significant fatigue, dizziness | Stop ascending. Consider descending 300-500m. Monitor closely for 24 hours. |
| Severe AMS | Intense headache, repeated vomiting, extreme fatigue, early confusion, breathlessness at rest | Descend immediately 500-1,000m. Do not wait. This is pre-HACE/HAPE territory. |
| HAPE | Breathlessness at rest, wet cough, gurgling breath, pink frothy sputum, cyanosis | EMERGENCY. Descend immediately. Nifedipine. Oxygen. Evacuate. |
| HACE | Confusion, ataxia (failed heel-to-toe test), hallucinations, altered consciousness | EMERGENCY. Descend immediately. Dexamethasone. Oxygen. Evacuate. |
Key distinction: Mild-to-moderate AMS is uncomfortable but manageable. The moment symptoms include breathlessness at rest, confusion, loss of coordination, or pink/frothy sputum, the situation has crossed from inconvenient to life-threatening.
Read our complete guide on altitude sickness signs and turnaround rules for detailed information on when to stop ascending.
Prevention Strategies
The best emergency is the one that never happens. HAPE and HACE are almost entirely preventable with proper planning and discipline.
Proper Acclimatization: Climb High, Sleep Low
The golden rule of altitude trekking is to give your body time to adapt. This means:
- Above 3,000m, increase sleeping altitude by no more than 300-500m per day
- Take a rest day every 3-4 days of ascent (or every 1,000m of altitude gained)
- Climb high, sleep low -- Day hikes to higher elevations followed by sleeping at lower camps allow your body to acclimatize without the stress of sleeping at the higher altitude
- Never sleep more than 600m higher than the previous night, regardless of how good you feel
On the EBC trek, this means taking acclimatization days in Namche Bazaar (3,440m) and Dingboche (4,410m). On the Annapurna Circuit, a rest day in Manang (3,540m) is essential. For the Manaslu Circuit, rest in Samagaun (3,530m) is mandatory.
See our detailed acclimatization guide for route-specific schedules.
Gradual Ascent Rate
The most common cause of HAPE and HACE is ascending too fast. Trekkers who fly into Lukla (2,860m) and push straight to Namche Bazaar in one day, or those who jeep to high trailheads and begin trekking immediately, are at highest risk.
- Allow at least 2 days to adjust at any new altitude band before ascending further
- If you fly into altitude (Lukla, Jomsom), plan extra acclimatization time
- Resist the urge to "keep up" with faster groups or stick to an overly ambitious itinerary
Hydration
Dehydration worsens the effects of altitude on the body. At altitude, you lose more water through respiration (dry air, increased breathing rate) and may not feel as thirsty as you should.
- Drink 3-4 liters of water per day above 3,000m
- Monitor urine color -- pale yellow indicates adequate hydration
- Avoid excessive alcohol (dehydrating and masks symptoms)
- Avoid excessive caffeine above 4,000m
Diamox (Acetazolamide) Prophylaxis
Diamox is a medication that accelerates acclimatization by stimulating breathing and reducing the likelihood of AMS, which in turn reduces the risk of progression to HAPE or HACE.
- Prophylactic dose: 125mg twice daily, starting 24 hours before ascent
- Continue until you have been at your highest altitude for 2-3 days, then taper
- Side effects: tingling in fingers/toes, increased urination, altered taste of carbonated drinks
- Diamox is not a treatment for HAPE or HACE -- it is a preventive measure for AMS
- Consult your doctor before taking Diamox, especially if you have sulfa allergies
See our complete Diamox guide for dosage details and contraindications.
Know Your Body, Do Not Push Through Symptoms
This is perhaps the most important prevention strategy and the one most often ignored:
- If you have AMS symptoms, do not ascend. Wait until symptoms resolve.
- If symptoms worsen at the same altitude, descend. Your body is telling you something.
- Do not let itinerary pressure override your health. Missing a day is better than missing your life.
- Do not compare yourself to others. Altitude susceptibility is individual and unpredictable.
Pro Tip
Medications for HAPE and HACE
These medications should be part of every high-altitude trekker's medical kit and should be carried by guides on treks above 4,000m. See our first aid kit guide for a complete list of recommended medications.
Nifedipine for HAPE
Nifedipine is a calcium channel blocker that dilates pulmonary blood vessels, reducing the pulmonary artery pressure that causes fluid leakage into the lungs.
- Dose: 20mg slow-release (extended-release formulation), every 6 hours
- Administration: Oral (swallowed whole, do not crush or chew the extended-release form)
- When to use: At the first signs of HAPE, while preparing for and during descent
- Side effects: Dizziness, low blood pressure, headache, flushing
- Caution: Can cause significant blood pressure drop -- the person should not stand up quickly
- Important: Nifedipine buys time for descent. It does NOT cure HAPE. You must still descend.
- Availability in Nepal: Available at pharmacies in Kathmandu and Pokhara. Purchase before your trek.
Dexamethasone for HACE
Dexamethasone is a powerful corticosteroid that reduces inflammation and brain swelling. It is the primary field medication for HACE.
- Dose: 8mg initial dose (oral or intramuscular), followed by 4mg every 6 hours
- Administration: Oral preferred. If the person is vomiting or unconscious, intramuscular injection if trained
- When to use: At the first signs of HACE (confusion, ataxia), while preparing for and during descent
- Side effects: Insomnia, mood changes, increased appetite, elevated blood sugar
- Duration: Continue until well below the altitude where symptoms began
- Important: Dexamethasone buys time for descent. It does NOT cure HACE. It can dramatically improve symptoms within hours, which creates a dangerous temptation to stop descending. Do not stop descending because the person "feels better" on Dexamethasone.
- Availability in Nepal: Available at pharmacies in Kathmandu. Some trekking agencies include it in their medical kits.
Critical Medication Notes
- These are emergency medications, not preventive treatments. Do not take them prophylactically for HAPE/HACE (Diamox is the prophylactic medication for AMS)
- They buy time for descent. The treatment for both conditions is getting lower, period.
- Carry them, but hope you never use them. Above 4,000m, having these medications in your pack or your guide's pack could save a life.
- Check expiration dates before your trek
- Know the correct doses and write them on the packaging
What Your Guide Should Know
If you are trekking with a guide (which is strongly recommended and required in many areas since 2026), your guide should be your first line of defense against altitude emergencies.
Red Flags That Your Guide Is Not Taking Altitude Seriously
Be concerned if your guide:
- Dismisses symptoms as "normal" and insists on continuing upward
- Has no medical training -- Reputable agencies train guides in altitude illness recognition and basic emergency response
- Does not carry emergency medications (Diamox, Dexamethasone, Nifedipine) on high-altitude treks
- Prioritizes the itinerary over health -- "We need to make it to camp today" should never override a trekker's worsening symptoms
- Does not know how to perform the ataxia test
- Has never dealt with an altitude emergency and does not know evacuation procedures
- Does not carry or know how to use a satellite phone or emergency communication device
What to Ask Your Guide Before the Trek
Before departing, ask your guide: "What would you do if someone in our group developed HAPE or HACE?" A competent guide should be able to describe the symptoms, explain that immediate descent is necessary, identify where the nearest HRA clinic or helicopter landing zone is, and show you the emergency medications they carry. If they cannot answer this question confidently, consider a different guide or agency.
Rescue and Evacuation Options in Nepal
When HAPE or HACE strikes and descent on foot is not feasible, knowing your evacuation options can save precious time.
Helicopter Rescue
Nepal has a well-established helicopter rescue system for trekkers, with helicopters based in Kathmandu and Lukla that can reach most trekking routes within 1-2 hours during good weather.
- Cost: $3,000-$7,000 USD depending on altitude and location
- Insurance: Ensure your travel insurance explicitly covers helicopter evacuation up to your maximum trekking altitude (minimum $100,000 coverage recommended)
- Limitations: Cannot fly in poor weather, at night, or above approximately 6,000m
- How to activate: Through your guide, lodge owner, or by contacting your insurance company's emergency line via satellite phone
Read our complete helicopter rescue guide for detailed information on how the process works.
Gamow Bag (Portable Altitude Chamber)
A Gamow bag is an inflatable, pressurized chamber that simulates descent by increasing air pressure around the patient. Spending 1-2 hours inside a Gamow bag is equivalent to descending approximately 1,500-2,000m.
- Available at: HRA clinics in Pheriche and Manang, some larger lodges on popular routes
- Use: For stabilizing a HAPE/HACE patient while arranging evacuation, or when descent is temporarily impossible
- Limitations: Requires constant pumping (exhausting work), symptoms often return when the person is removed, not a substitute for actual descent
Himalayan Rescue Association (HRA) Clinics
The HRA operates two high-altitude medical clinics on Nepal's most popular trekking routes:
-
Pheriche Clinic (4,371m): On the Everest Base Camp route, staffed by volunteer physicians during the main trekking seasons (March-May and September-November). Provides altitude illness diagnosis and treatment, supplemental oxygen, and Gamow bag therapy.
-
Manang Clinic (3,540m): On the Annapurna Circuit, similarly staffed during trekking seasons. Offers daily altitude sickness lectures that every Circuit trekker should attend.
Both clinics provide free altitude sickness lectures and consultations. They charge for medications and extended treatment.
Pro Tip
Real Scenarios: What Can Go Wrong and What to Do
The following are composite scenarios based on real events reported by the Himalayan Rescue Association and trekking agencies. Names and specific details have been changed.
Scenario 1: HAPE on the EBC Trek
A 32-year-old trekker arrived in Dingboche (4,410m) after skipping the recommended acclimatization day in Namche Bazaar. She felt fine that afternoon. During the night, she developed a dry cough and felt unable to get comfortable. By morning, she was breathless sitting up in bed and could hear a crackling sound when she breathed deeply.
What went right: Her roommate recognized the symptoms from a pre-trek altitude sickness briefing and immediately woke their guide. The guide recognized HAPE, administered oxygen from the lodge's supply, gave her Nifedipine, and organized porters to carry her down to Pheriche where the HRA clinic was open. By the time she reached Pheriche (just 4 hours later and 40m lower, plus medical attention), her breathing had improved significantly. She was evacuated by helicopter to Kathmandu the next morning.
What could have gone wrong: If the roommate had let her "sleep it off," the fluid accumulation could have become fatal by late morning.
Scenario 2: HACE on the Annapurna Circuit
A 45-year-old trekker had been experiencing headaches since arriving in Manang (3,540m), which he managed with ibuprofen. At Thorong La High Camp (4,925m), his companions noticed he was unusually quiet during dinner and seemed confused about the plan for the next day. When asked to walk heel-to-toe, he could not complete three steps without stumbling.
What went right: Despite the trekker insisting he was "just tired" and would "be fine after sleep," his companions and guide recognized these as HACE symptoms. They began descent at 8 PM in darkness with headlamps, reaching Thorong Phedi (4,450m) by 10 PM. After Dexamethasone administration, the trekker's condition stabilized overnight. He was further evacuated to Manang and then to Kathmandu by helicopter.
What could have gone wrong: If the group had waited until morning to descend, the trekker may have been unconscious by dawn. The nighttime descent, though difficult and uncomfortable, likely saved his life.
Scenario 3: Combined HAPE and HACE
A 28-year-old trekker on the Manaslu Circuit developed a persistent cough at Samdo (3,860m) that worsened at Dharamsala (4,460m). By 2 AM, she was breathless, coughing pink frothy sputum, and when her guide checked on her, she was confused and could not recognize where she was.
What went right: The guide immediately recognized combined HAPE/HACE. He administered both Nifedipine and Dexamethasone, propped her up in a sitting position, and at first light used a satellite phone to call for helicopter evacuation. A helicopter reached Dharamsala by 7 AM and evacuated her to Kathmandu. She spent three days in hospital and made a full recovery.
What was critical: The guide carried both medications and a satellite phone, recognized the severity immediately, and did not waste time hoping for improvement.
After a HAPE or HACE Episode
Immediate Aftermath
- Do not re-ascend on the same trip. This is non-negotiable. The risk of recurrence on the same trip is extremely high.
- Seek medical evaluation at a hospital in Kathmandu or Pokhara, even if you feel better
- Rest at low altitude for a minimum of 3-5 days before any physical activity
- Hydrate and eat well to support recovery
Long-Term Considerations
- Medical clearance: Before any future high-altitude trekking, obtain clearance from a doctor experienced in altitude medicine
- History of HAPE: Recurrence rate is approximately 60% on subsequent high-altitude exposure. You can trek at altitude again, but with greater caution, slower ascent rate, and potentially prophylactic Nifedipine
- History of HACE: Recurrence risk is lower than HAPE but still significant. Very conservative ascent profiles and acclimatization schedules are essential
- Consider altitude susceptibility testing: Some specialist centers offer hypoxic challenge tests that can indicate your individual susceptibility
- Inform future guides: Always tell trekking agencies and guides about previous HAPE/HACE episodes
Frequently Asked Questions
What is the difference between HAPE and HACE?
HAPE (High Altitude Pulmonary Edema) is fluid in the lungs -- the hallmark signs are breathlessness, a worsening cough, and in severe cases pink frothy sputum. HACE (High Altitude Cerebral Edema) is swelling in the brain -- the hallmark signs are confusion, loss of coordination (a failed heel-to-toe ataxia test), and altered behavior. Both are life-threatening, both require immediate descent, but the field medications differ: Nifedipine for HAPE, Dexamethasone for HACE.
How far down do I need to descend?
For a confirmed HAPE or HACE emergency, aim to lose at least 500-1,000m of elevation. Improvement often begins after just 300-600m, but do not stop the moment someone "feels better" -- keep descending until the person is well below the altitude where symptoms started, and seek medical care.
Can fit, young people get HAPE or HACE?
Yes, absolutely. Physical fitness provides zero protection against HAPE or HACE. In fact, some studies suggest that young, fit individuals are at slightly higher risk because they tend to ascend faster and push harder. HAPE and HACE have killed elite athletes, military personnel, and experienced mountaineers.
How quickly do HAPE and HACE develop?
HAPE typically develops over 2-4 days at altitude, often worsening overnight. HACE can develop over hours to days, sometimes progressing rapidly from mild AMS to severe HACE in under 12 hours. Both can progress from manageable to life-threatening in a matter of hours once the severe phase begins.
Can I prevent HAPE/HACE with Diamox?
Diamox (Acetazolamide) helps prevent AMS, which reduces the risk of progression to HAPE or HACE. However, Diamox is not a direct treatment for HAPE or HACE. See our Diamox guide for details. The primary prevention is proper acclimatization and gradual ascent.
What if descent is impossible (weather, darkness, terrain)?
If immediate descent is truly impossible, use all available stopgap measures: administer the appropriate medications (Nifedipine for HAPE, Dexamethasone for HACE, both if needed), provide supplemental oxygen if available, use a Gamow bag if one is accessible, and descend at the very first opportunity. In most cases, some descent is possible even in difficult conditions and should be attempted.
Should I carry Nifedipine and Dexamethasone on my trek?
If you are trekking above 4,000m, yes. These medications are lightweight, inexpensive, and could save your life or someone else's. Ensure your guide also carries them. Purchase them from pharmacies in Kathmandu before your trek and confirm the correct dosages with a doctor.
How do I know if it is bad AMS or actual HACE?
The key distinguishing features of HACE versus severe AMS are: confusion or altered mental status, inability to walk heel-to-toe (failed ataxia test), and personality or behavior changes. If any of these are present alongside AMS symptoms, treat it as HACE and descend immediately.
Can I get HAPE at altitudes below 3,000m?
Rarely, but it has been documented. Most HAPE cases occur above 3,000m, with risk increasing significantly above 4,000m. However, individuals with a history of HAPE or certain cardiovascular conditions may be susceptible at lower altitudes.
What if the affected person refuses to descend?
This is common with HACE because the condition impairs judgment. The person may insist they are fine or become combative. Their companions and guide must make the decision for them. A HACE patient's judgment cannot be trusted. Document your observations, explain the situation calmly but firmly, and begin descent even if the person protests.
How much does helicopter rescue cost in Nepal?
Helicopter rescue typically costs $3,000-$7,000 USD depending on altitude, location, and how far you must be flown (a short evacuation from the Everest region to Lukla sits at the lower end, while a flight all the way to Kathmandu costs more). This is why proper travel insurance is absolutely essential. Ensure your policy explicitly covers helicopter evacuation up to your maximum trekking altitude.
Can I trek again after a HAPE or HACE episode?
Yes, with proper precautions. Many people who have experienced HAPE or HACE return to high-altitude trekking successfully. However, you should: obtain medical clearance, ascend very conservatively, consider prophylactic medication, inform your guide of your history, and be prepared to turn back at the first sign of recurrence. The mountains will always be there for another attempt.
Are there early warning devices or oximeters I should carry?
A pulse oximeter is a small, inexpensive device that measures blood oxygen saturation (SpO2). While not diagnostic on its own, a SpO2 reading below 80% at altitude, or a significant drop from your personal baseline, can be an early warning of HAPE. Many experienced trekkers and guides carry them. However, do not rely solely on numbers -- clinical symptoms always take priority.
What happens at the HRA clinics in Pheriche and Manang?
The Himalayan Rescue Association clinics provide altitude sickness diagnosis, treatment, supplemental oxygen, Gamow bag therapy, and emergency stabilization. They are staffed by volunteer physicians during the trekking season (typically March-May and September-November). They also provide free daily altitude sickness lectures. Consultations are free; medications and extended treatment are charged.
Final Thoughts: Knowledge Is Your Best Protection
HAPE and HACE are terrifying conditions, but they are also predictable and preventable. The trekkers who get into trouble are almost always those who ascend too fast, ignore warning symptoms, or prioritize their itinerary over their health.
Your best protection is threefold:
- Acclimatize properly -- Follow the rules for gradual ascent, take rest days, and use proven acclimatization strategies
- Recognize symptoms early -- Know the difference between normal AMS and danger signs, and perform the ataxia test when in doubt
- Act decisively -- When symptoms cross the threshold from uncomfortable to dangerous, descend immediately without hesitation or delay
Nepal's Himalayas offer some of the most extraordinary trekking on Earth. With proper knowledge and respect for altitude, you can experience these mountains safely and return home with stories of triumph rather than tragedy.
For a comprehensive overview of all altitude-related illnesses, see our main altitude sickness prevention and treatment guide. For route-specific acclimatization schedules, see our acclimatization guide.