


2,500m (8,200 ft)
5,364m (17,598 ft)
50-85% of trekkers above 4,500m experience symptoms
Can be fatal within 12-24 hours if untreated
Immediate descent (500-1,000m minimum)
Ascend no more than 300-500m sleeping altitude per day above 3,000m
Altitude sickness is the single greatest medical threat facing trekkers in Nepal. Every year, the Himalayan Rescue Association treats hundreds of cases at their high-altitude clinics in Pheriche (4,371m) and Manang (3,540m), and dozens of trekkers require emergency helicopter evacuation. Some don't survive.
The tragedy is that nearly every altitude-related death is preventable. With proper knowledge, appropriate acclimatization schedules, early symptom recognition, and willingness to descend when necessary, you can trek safely to Nepal's highest destinations. This comprehensive guide provides everything you need to understand, prevent, recognize, and respond to altitude illness.
This guide covers:
- Understanding altitude zones and how your body responds
- The three types of altitude illness (AMS, HACE, HAPE) and their symptoms
- Golden rules of acclimatization that can save your life
- Critical turnaround rules and when to descend
- Prevention strategies and medication protocols
- Trek-specific altitude considerations for Nepal's major routes
- Emergency evacuation procedures
Whether you're planning Everest Base Camp, the Annapurna Circuit, or any other high-altitude trek in Nepal, this information is essential reading before you set foot on the trail.
Table of Contents
- Why Altitude Sickness Matters in Nepal
- Understanding Altitude Zones
- Three Types of Altitude Illness
- The Golden Rules of Acclimatization
- Symptom Recognition Checklist
- Critical Turnaround Rules
- Prevention Strategies
- Dehydration Warning Signs & Prevention
- Medication Guide
- Treatment Protocols
- Trek-Specific Altitude Considerations
- Emergency Evacuation
- Frequently Asked Questions
Why Altitude Sickness Matters in Nepal
Nepal's trekking routes reach some of the highest altitudes accessible to non-mountaineers. The Everest Base Camp trek reaches 5,364m, the Three Passes trek exceeds 5,500m multiple times, and even the popular Annapurna Circuit crosses Thorong La at 5,416m. At these elevations, the atmospheric pressure is roughly half what it is at sea level, meaning each breath delivers only half the oxygen your body is accustomed to.
The Statistics Paint a Stark Picture
Research conducted in the Khumbu region reveals the scope of the problem:
- 50-85% of trekkers ascending above 4,500m experience at least mild AMS symptoms
- 1-2% of trekkers develop life-threatening HACE or HAPE
- Approximately 4-6 trekkers die annually from altitude-related illness in Nepal (official statistics likely undercount actual numbers)
- 84% of altitude-related deaths occur in people who ignored warning symptoms and continued ascending
- The average helicopter evacuation from the Everest region costs $3,000-5,000 USD
Who Is at Risk?
A critical truth about altitude sickness: it does not discriminate based on fitness level. In fact, highly fit individuals sometimes face greater risk because they're tempted to push through symptoms that would stop less fit trekkers.
Risk factors include:
- Rapid ascent rate (the most significant factor)
- History of previous altitude illness
- Sleeping at high altitude without acclimatization
- Dehydration
- Respiratory infections
- Certain pre-existing conditions
- Individual physiological susceptibility (partly genetic, unpredictable)
Not reliably predictive:
- Age (within normal trekking ranges)
- Sex
- Physical fitness level
- Prior high-altitude experience (though it provides some insight)
The Fitness Trap
Marathon runners, professional athletes, and extremely fit individuals die from altitude sickness every year. High fitness can mask early symptoms and enable faster ascent rates that outpace acclimatization. Your lungs and cardiovascular system may be exceptional, but your cells still need time to adapt to lower oxygen availability. Never assume fitness provides protection.
The Life-Saving Truth
Here's the most important thing to understand: altitude sickness is almost entirely preventable and nearly always treatable if caught early. The treatment is straightforward—stop ascending or descend. The challenge is psychological: convincing yourself to turn around when you've invested time, money, and emotional energy into reaching a destination.
The trekkers who die from altitude illness are almost never those who didn't know the symptoms. They're the ones who knew the symptoms, recognized them, and chose to continue anyway. This guide can give you knowledge, but you must supply the wisdom to act on it.
Understanding Altitude Zones
Not all altitude is equal in terms of physiological stress. Understanding the altitude zones helps you anticipate where symptoms might emerge and how your body needs to adapt at different elevations.
Altitude Classification
| Zone | Elevation | Physiological Response | Nepal Trekking Context |
|---|---|---|---|
| Low Altitude | 0-1,500m (0-4,900 ft) | Normal oxygen saturation. No acclimatization needed. | Kathmandu (1,400m), Pokhara (800m) |
| Moderate Altitude | 1,500-2,500m (4,900-8,200 ft) | Minor effects possible. Most people adapt easily. | Lukla (2,860m), early Annapurna trail |
| High Altitude | 2,500-3,500m (8,200-11,500 ft) | AMS symptoms can begin. Acclimatization becomes important. | Namche Bazaar (3,440m), Manang (3,540m) |
| Very High Altitude | 3,500-5,500m (11,500-18,000 ft) | AMS common without proper acclimatization. HACE/HAPE risk increases. | Dingboche (4,410m), Gorak Shep (5,164m), Thorong La (5,416m) |
| Extreme Altitude | Above 5,500m (18,000 ft) | Progressive deterioration inevitable. Acclimatization maxes out. | EBC (5,364m), Kala Patthar (5,545m), high passes |
What Happens to Your Body at Altitude
When you ascend to high altitude, several physiological changes occur:
Immediate responses (first hours):
- Increased breathing rate and depth (hyperventilation)
- Increased heart rate
- Decreased blood oxygen saturation (SpO2)
- Mild fluid shifts causing peripheral edema
Short-term adaptations (days to weeks):
- Continued hyperventilation (becomes more efficient)
- Increased red blood cell production (begins around day 3-4)
- Improved oxygen extraction efficiency
- Metabolic adjustments in cells
- Kidney adjustments to blood chemistry
The acclimatization timeline:
- Days 1-3: Initial stress response, symptoms most likely to emerge
- Days 4-7: Early adaptation, symptoms often improve
- Days 7-14: Significant adaptation occurs
- Beyond 2 weeks: Well-adapted to current altitude, but still vulnerable to rapid further ascent
Understanding Oxygen Saturation
At sea level, healthy blood oxygen saturation (SpO2) is 95-100%. At Everest Base Camp altitude, well-acclimatized trekkers typically show SpO2 of 75-85%. This is normal and expected. What matters more than absolute numbers is your trend and how you feel. A fit, acclimatized person at 80% SpO2 who feels fine is healthier than someone at 85% with a splitting headache and confusion.
Key Altitude Thresholds for Nepal Trekkers
| Threshold | Significance |
|---|---|
| 2,500m | Altitude illness becomes possible. Pay attention to how you feel. |
| 3,000m | "Rule of 300" applies—increase sleeping altitude by no more than 300-500m per day |
| 4,000m | Mandatory acclimatization days should be built into itinerary |
| 5,000m | Multiple acclimatization days required. High risk zone for HACE/HAPE |
| 5,500m+ | Extreme altitude—body cannot fully acclimatize, progressive deterioration begins |
Three Types of Altitude Illness
Altitude illness exists on a spectrum from mild to life-threatening. Understanding the three main forms—AMS, HACE, and HAPE—helps you recognize where you are on that spectrum and respond appropriately.
Acute Mountain Sickness (AMS)
AMS is the mildest and most common form of altitude illness. It's your body signaling that it's struggling to adapt and needs more time. While uncomfortable, AMS itself is not immediately dangerous—but it demands attention because it can progress to HACE or HAPE.
When it appears: Typically 6-24 hours after arrival at a new altitude
Core symptoms (must have headache plus at least one other):
- Headache (the defining symptom—present in almost all AMS cases)
- Fatigue or weakness
- Dizziness or lightheadedness
- Nausea, with or without vomiting
- Loss of appetite
- Difficulty sleeping (insomnia, frequent waking, disturbed sleep)
What it feels like: Many describe AMS as feeling like a hangover or the early stages of flu. The headache is typically dull, persistent, and worsens with exertion, coughing, or bending over.
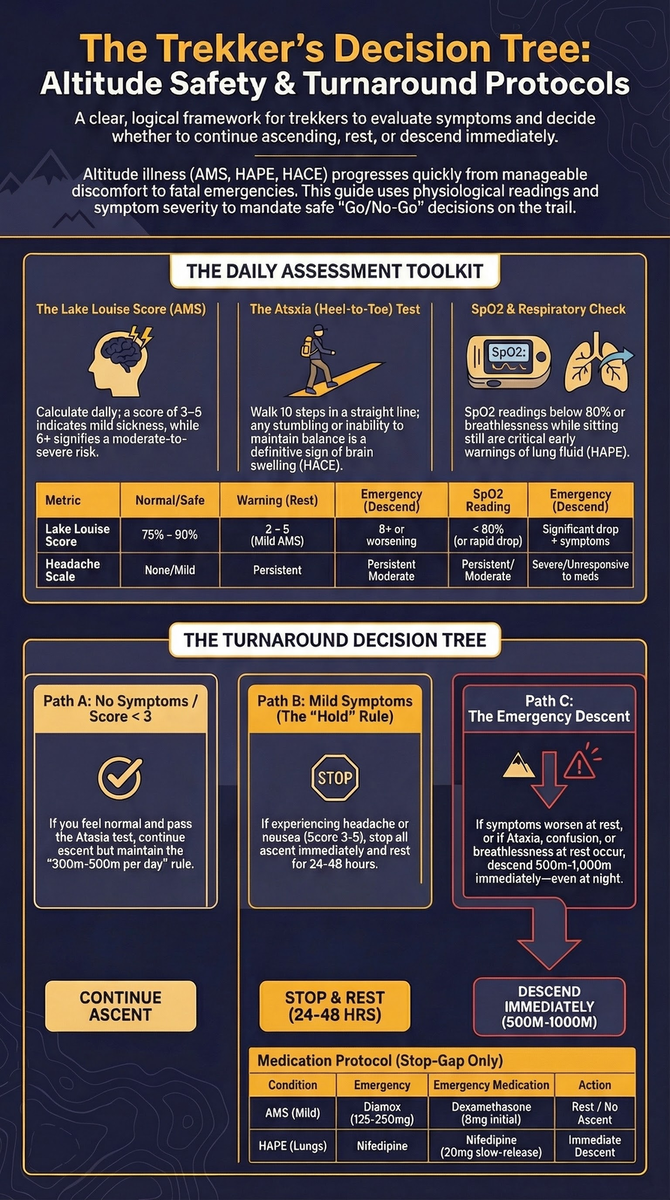
Lake Louise AMS Score
The Lake Louise Acute Mountain Sickness Score is the international standard for assessing AMS severity. It provides an objective measure that helps distinguish mild from moderate cases.
Scoring system:
| Symptom | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| Headache | None | Mild | Moderate | Severe, incapacitating |
| GI symptoms | Good appetite | Poor appetite or nausea | Moderate nausea or vomiting | Severe nausea/vomiting, incapacitating |
| Fatigue/weakness | Not tired | Mild fatigue | Moderate fatigue | Severe fatigue, incapacitating |
| Dizziness | None | Mild | Moderate | Severe, incapacitating |
| Sleep quality | Slept well | Did not sleep as well as usual | Woke many times, poor sleep | Could not sleep at all |
Interpretation:
- Score 3-5: Mild AMS. Do not ascend until symptoms resolve.
- Score 6+: Moderate to severe AMS. Consider descent. Do not ascend under any circumstances.
- Any score with symptoms not improving or worsening: Descent required.
Pro Tip
Perform the Lake Louise assessment on yourself every evening at altitude. Write down your scores in a notebook. This creates an objective record that helps you recognize trends—a score of 4 that was 2 yesterday is more concerning than a steady 4 that's been improving from 6.
High Altitude Cerebral Edema (HACE)
HACE is AMS that has progressed to involve swelling of the brain. It's a life-threatening emergency. Without descent, HACE is fatal within 24-72 hours. Even with treatment, permanent neurological damage can occur.
Key warning signs:
- Ataxia (loss of coordination)—the hallmark sign of HACE
- Severe, unrelenting headache not responsive to medication
- Confusion, disorientation, or altered mental status
- Drowsiness, lethargy, or difficulty staying awake
- Personality changes (irritability, withdrawal, uncharacteristic behavior)
- Visual disturbances
- Nausea and vomiting
- In advanced cases: hallucinations, coma
The Ataxia Test: Your Critical Warning System
The heel-to-toe walk (tandem gait) test is the most reliable field indicator of HACE. Here's how to perform it:
- Draw a straight line on the ground (or use a crack between stones)
- Walk heel-to-toe along the line for 10 steps, as if on a tightrope
- A healthy person can do this easily
- Someone developing HACE will wobble, step off the line, or be unable to complete the test
If you or anyone in your group fails the ataxia test, treat it as a medical emergency. Descent must begin immediately, even at night.
HACE progression timeline:
- Can develop from AMS within 12-24 hours
- Once ataxia appears, condition can deteriorate within hours
- Without descent, death typically occurs within 1-3 days
- Even with descent, full recovery may take days to weeks
Risk factors for AMS progressing to HACE:
- Continuing to ascend with AMS symptoms
- Sleeping at higher altitude despite symptoms
- Rapid ascent rate
- History of previous HACE
- Possibly genetic susceptibility
High Altitude Pulmonary Edema (HAPE)
HAPE is fluid accumulation in the lungs. It can develop independently of AMS or alongside it. HAPE is the most common cause of death from altitude illness and can kill within 12 hours if untreated.
Key warning signs:
- Persistent dry cough, often progressing to produce pink, frothy sputum
- Shortness of breath at rest (not just during exertion)
- Extreme fatigue and weakness disproportionate to exertion
- Chest tightness, congestion, or gurgling sensation
- Rapid heart rate (tachycardia)
- Cyanosis (blue/gray discoloration of lips, fingernails)
- Rattling or crackling sound when breathing (rales)
- In advanced cases: inability to lie flat, severe respiratory distress
The "performance gap" warning sign:
One of the earliest indicators of developing HAPE is a sudden, unexplained decline in performance. If someone who was keeping pace yesterday is now struggling to keep up, breathing heavily, and needing frequent rests, HAPE may be developing—even before classic symptoms appear.
HAPE Emergency Recognition
These symptoms indicate advanced HAPE requiring immediate action:
- Breathless at rest (not just with exertion)
- Unable to complete sentences without pausing for breath
- Coughing up pink or bloody fluid
- Audible gurgling or crackling from chest
- Confusion combined with respiratory symptoms
- Blue lips or fingernails
HAPE can kill within 12 hours. Descent must begin immediately. Every hour of delay increases mortality risk.
Why HAPE is particularly dangerous:
- Can develop rapidly (sometimes within hours)
- Early symptoms often mistaken for fatigue or "Khumbu cough"
- Can occur independently of AMS (you can feel otherwise "fine")
- Worsens rapidly once established
- Requires significant descent (1,000m+ ideally) for meaningful improvement
HAPE risk factors:
- Previous episode of HAPE (strongest predictor)
- Rapid ascent
- Heavy exertion at altitude
- Pre-existing respiratory conditions
- Recent upper respiratory infection
- Cold exposure
- Possibly genetic factors
Comparing the Three Conditions
| Feature | AMS | HACE | HAPE |
|---|---|---|---|
| Primary system affected | General / Neurological | Brain | Lungs |
| Cardinal symptom | Headache | Ataxia (loss of coordination) | Breathlessness at rest |
| Onset timing | 6-24 hours after arrival | Typically follows AMS | Can be independent or with AMS |
| Progression speed | Hours to days | Hours once established | Hours (can be very rapid) |
| Without treatment | Usually self-limiting | Fatal in 1-3 days | Fatal in 12-72 hours |
| Treatment | Rest, no ascent, consider descent | IMMEDIATE descent + medications | IMMEDIATE descent + oxygen |
| Common altitude of occurrence | Above 2,500m | Usually above 4,000m | Usually above 3,000m |
The Golden Rules of Acclimatization
Proper acclimatization is your primary defense against altitude illness. These rules, developed over decades of mountain medicine research, can reduce your AMS risk by 80% or more.
Rule 1: Climb High, Sleep Low
This principle maximizes your altitude exposure while minimizing overnight stress. During the day, hike to higher elevations to stimulate acclimatization, then descend to sleep at a lower altitude where your body can recover more effectively.
Practical application:
- On acclimatization days, hike 300-500m above your sleeping altitude
- Return to your accommodation at lower elevation for sleep
- Example at Namche (3,440m): Day hike to Everest View Hotel (3,880m), sleep in Namche
- Example at Dingboche (4,410m): Day hike toward Nangkartshang Peak (4,800m), sleep in Dingboche
Rule 2: The 300-500m Rule
Above 3,000m, increase your sleeping altitude by no more than 300-500m per day. This gives your body adequate time to adapt before each new stress.
Standard conservative guidelines:
- Maximum 300m sleeping altitude gain per day (safest approach)
- Maximum 500m sleeping altitude gain per day (acceptable for most)
- Never exceed 600m sleeping altitude gain in a single day
What this looks like on the EBC trek:
| Day | From | To | Sleeping Altitude Gain |
|---|---|---|---|
| 3 | Phakding (2,610m) | Namche (3,440m) | +830m (high—built-in rest day follows) |
| 4 | Namche | Namche (acclimatization) | 0m |
| 5 | Namche (3,440m) | Tengboche (3,870m) | +430m |
| 6 | Tengboche (3,870m) | Dingboche (4,410m) | +540m (borderline—consider rest day) |
| 7 | Dingboche | Dingboche (acclimatization) | 0m |
| 8 | Dingboche (4,410m) | Lobuche (4,940m) | +530m |
| 9 | Lobuche (4,940m) | Gorak Shep (5,164m) | +224m |
Rule 3: Schedule Mandatory Acclimatization Days
For every 1,000m gained in sleeping altitude above 3,000m, schedule a rest day. These aren't optional—they're essential safety components of your itinerary.
Recommended acclimatization day schedule:
| Altitude Zone | Acclimatization Day Recommendation |
|---|---|
| 3,000-3,500m | First night above 3,000m: consider rest day |
| 3,500-4,000m | Mandatory rest day (e.g., Namche at 3,440m) |
| 4,000-4,500m | Mandatory rest day (e.g., Dingboche at 4,410m) |
| 4,500-5,000m | Consider additional rest day before final push |
| Above 5,000m | Minimize time; descend to sleep lower if possible |
What to do on acclimatization days:
- Wake naturally, don't force early starts
- Eat breakfast, hydrate well
- Do a 2-4 hour day hike to a higher point
- Climb 300-500m above sleeping altitude
- Descend for lunch
- Rest in afternoon
- Early dinner and sleep
- Monitor symptoms (Lake Louise scoring)
Pro Tip
Acclimatization days are not "wasted" days. They're when your body does its most important adaptation work. Trekkers who rush through without rest days have dramatically higher rates of AMS, evacuation, and failed summit attempts. The "extra" days often mean the difference between reaching your destination and having to turn back.
Rule 4: Hydrate Aggressively
At altitude, you lose more fluid through respiration (the air is dry, and you breathe more) and may not feel as thirsty as you should. Dehydration worsens AMS symptoms and impairs acclimatization.
Hydration targets:
- Minimum 3-4 liters per day at altitude
- 4-5 liters on active trekking days
- Urine should be light yellow to clear
- Dark urine indicates dehydration
Hydration tips:
- Start drinking before you feel thirsty
- Carry 2 x 1-liter bottles and drink regularly
- Include electrolytes (sports drinks, ORS, or tablets)
- Hot drinks count—tea houses make this easy
- Avoid alcohol (see below)
- Wake at night to urinate? Good—it means you're hydrating properly
Rule 5: Avoid Alcohol and Sleeping Pills
Alcohol:
- Depresses respiratory drive, reducing oxygen intake during sleep
- Causes dehydration
- Masks early symptoms
- Impairs judgment about symptoms
- Recommendation: Completely avoid alcohol above 3,000m
Sleeping pills (including Ambien, Valium, other sedatives):
- Depress respiratory drive significantly
- Reduce breathing rate and depth during sleep
- Dangerous combination with low oxygen environment
- Can mask HACE symptoms
- Recommendation: Never use above 3,000m
What about Diamox? Diamox (acetazolamide) is NOT a sleeping pill—it works differently and actually helps acclimatization. See the Medication Guide section below.
Rule 6: Never Ascend with Symptoms
This rule is absolute. If you have AMS symptoms—any symptoms—do not climb to a higher sleeping altitude. The options are:
- Rest at current altitude until symptoms resolve completely
- Descend if symptoms worsen or don't improve within 24-48 hours
The logic is simple: AMS symptoms mean your body isn't keeping up with current altitude stress. Adding more stress by climbing higher dramatically increases the risk of progression to HACE or HAPE.
Rule 7: Eat Well and Sleep Well
Nutrition at altitude:
- Your metabolism increases 10-30% at altitude
- Eat carbohydrates—they require less oxygen to metabolize than fats or proteins
- Don't skip meals, even if appetite is reduced
- Dal bhat (rice and lentils) is ideal high-altitude fuel
- Avoid heavy, fatty foods
Sleep at altitude:
- Sleep quality naturally decreases at altitude
- Periodic breathing (Cheyne-Stokes respiration) is common and not dangerous
- Sleep with head slightly elevated if possible
- Don't use sleeping pills (see above)
- If severely unable to sleep, this may be an AMS symptom
Summary: The Seven Golden Rules
- Climb high, sleep low on acclimatization days
- Gain no more than 300-500m sleeping altitude per day above 3,000m
- Take mandatory rest days every 1,000m gained
- Drink 3-4 liters minimum per day
- Avoid alcohol and sleeping pills above 3,000m
- Never ascend with symptoms—rest or descend
- Eat well and prioritize sleep quality
Symptom Recognition Checklist
Early recognition of altitude illness symptoms allows early intervention—and early intervention prevents serious outcomes. Use this comprehensive checklist to monitor yourself and fellow trekkers.
Daily Symptom Assessment
Perform this assessment every evening before sleep and every morning after waking:
Headache:
- None (0 points)
- Mild headache (1 point)
- Moderate headache (2 points)
- Severe, incapacitating headache (3 points)
Gastrointestinal:
- Good appetite, no nausea (0 points)
- Reduced appetite or mild nausea (1 point)
- Moderate nausea or vomiting (2 points)
- Severe nausea/vomiting (3 points)
Fatigue:
- Normal energy (0 points)
- Mildly tired (1 point)
- Very tired, weak (2 points)
- Extremely fatigued, unable to continue (3 points)
Dizziness:
- None (0 points)
- Mild dizziness (1 point)
- Moderate dizziness (2 points)
- Severe dizziness (3 points)
Sleep (previous night):
- Slept well (0 points)
- Did not sleep as well as usual (1 point)
- Woke many times, poor sleep (2 points)
- Could not sleep at all (3 points)
Warning Signs Requiring Immediate Attention
HACE Warning Signs (any one requires immediate descent):
- Cannot walk in a straight line (heel-to-toe test failure)
- Confusion or disorientation
- Uncharacteristic behavior changes
- Severe headache not relieved by medication
- Drowsiness, difficulty staying awake
- Vision changes
HAPE Warning Signs (any one requires immediate descent):
- Breathless at rest (not just with exertion)
- Cannot keep pace with yesterday's performance
- Persistent cough with pink/bloody sputum
- Gurgling or crackling sounds from chest
- Chest tightness that doesn't improve with rest
- Blue lips or fingernails
Symptom Severity Guide
| Severity Level | Symptoms Present | Required Action |
|---|---|---|
| None | Lake Louise Score 0-2, feeling good | Continue normal ascent schedule |
| Mild AMS | Score 3-5, headache with minor symptoms | Do NOT ascend. Rest at current altitude. Monitor closely. |
| Moderate AMS | Score 6+, multiple significant symptoms | Strong consideration for descent. Absolutely no ascent. |
| Severe AMS / Probable HACE | Ataxia, confusion, severe symptoms | DESCEND IMMEDIATELY. This is an emergency. |
| Probable HAPE | Breathless at rest, cough with bloody sputum | DESCEND IMMEDIATELY. Administer oxygen if available. |
Critical Turnaround Rules
Knowing when to stop, rest, or descend is the most important decision you'll make at altitude. These rules provide clear guidance for different scenarios.
When to Stop Ascending (Hold at Current Altitude)
Stop and spend an extra night at your current altitude if:
- You have any AMS symptoms (Lake Louise Score 3+)
- You feel "off" or not yourself
- You're significantly more fatigued than expected
- You have a persistent headache
- Sleep was severely disturbed
- Appetite is significantly reduced
- You've gained more than 500m sleeping altitude in 24 hours
Action plan when stopping:
- Rest and hydrate
- Do a short acclimatization hike (climb high, return low)
- Monitor symptoms using Lake Louise scoring
- Continue upward only when symptoms fully resolve
- If symptoms persist or worsen after 24-48 hours, descend
When to Descend Immediately
Immediate Descent Triggers
Descend immediately if you or anyone in your group experiences:
- Ataxia (failed heel-to-toe walking test)
- Confusion, disorientation, or altered mental status
- Severe headache unresponsive to medication
- Shortness of breath at rest
- Coughing up pink or bloody sputum
- Lake Louise Score increasing despite rest
- Any symptom that worsens despite 24 hours at same altitude
- Worsening symptoms during the night
"When in doubt, go down"—this mantra saves lives.
How Far to Descend
For Mild AMS (stopped worsening):
- Descend 500m minimum
- Often resolves within hours of descent
- Can attempt re-ascent after 24-48 hours of no symptoms
For Moderate AMS:
- Descend 500-1,000m
- May need 1-2 days recovery before considering re-ascent
- Re-ascend more slowly
For HACE or HAPE:
- Descend as far as possible—ideally 1,000m+ minimum
- Continue descending until symptoms improve significantly
- Evacuation likely required
- May need days to weeks of recovery before high altitude exposure
The "Never" Rules
NEVER:
- Ascend with any AMS symptoms
- Assume symptoms will improve with more ascent
- Let group pressure override your body's signals
- Believe "I just need to push through"
- Ascend if you failed the ataxia test
- Stay high with worsening symptoms to wait for morning
- Leave a symptomatic person alone
Night Descent: When to Go in the Dark
Normally, night travel in the mountains is dangerous and avoided. However, altitude emergencies are an exception.
Descend at night if:
- Someone shows HACE signs (ataxia, confusion)
- Someone shows HAPE signs (breathless at rest, bloody sputum)
- Symptoms are rapidly worsening
- You believe someone may die before morning
Night descent protocol:
- Send someone ahead to arrange help at lower altitude
- Use headlamps, go slowly on terrain
- Keep the patient between two healthy people
- Descend as far as possible, minimum 500m
- Call for helicopter evacuation if available
- Continue at first light if still above danger zone
Pro Tip
A person with severe altitude illness will almost always feel better and become more able to walk as they descend. Even 200-300m of descent can produce noticeable improvement. Use this to your advantage—start descending and the patient will become more helpful in their own evacuation.
Prevention Strategies
The best treatment for altitude illness is preventing it in the first place. These strategies, combined with the golden rules of acclimatization, dramatically reduce your risk.
Pre-Trek Preparation
Physical fitness:
- Begin training 3-4 months before trek
- Focus on cardiovascular endurance
- Include hiking with elevation gain
- Simulate pack weight during training
- Fitness doesn't prevent AMS but aids overall trek success
Medical preparation:
- Consult your doctor about altitude medication
- Get any recommended vaccinations
- Address pre-existing conditions
- Obtain prescription for Diamox if appropriate
- Ensure travel insurance covers high-altitude evacuation
Pre-acclimatization (if possible):
- Spend time above 2,500m in the weeks before your trek
- Even one night at 3,000m can help
- Consider arriving in Nepal early and trekking at moderate altitude first
- The Langtang Valley or Poon Hill can serve as acclimatization precursors
Optimal Itinerary Design
Choose itineraries with:
- Mandatory acclimatization days built in
- Gradual altitude gain (300-500m/day max sleeping altitude)
- "Climb high, sleep low" opportunities
- Flexibility for additional rest days
- Descent options at critical points
Red flags in itineraries:
- No rest days above 3,500m
- Gains of 600m+ sleeping altitude in single days
- Fixed schedules with no flexibility
- "Speed" itineraries that cut standard acclimatization
Recommended vs. risky schedules:
| Destination | Recommended Duration | Minimum Safe Duration | Too Fast |
|---|---|---|---|
| EBC | 14-16 days | 12-13 days | Under 11 days |
| Three Passes | 18-21 days | 16-17 days | Under 15 days |
| Annapurna Circuit | 14-18 days | 12-14 days | Under 11 days |
| Manaslu Circuit | 15-18 days | 14 days | Under 13 days |
Daily Prevention Habits
Every day at altitude:
- Hydrate: 3-4 liters minimum, more on active days
- Assess: Check symptoms using Lake Louise scoring
- Communicate: Tell your guide and group how you feel honestly
- Pace yourself: Walk slowly, rest frequently
- Eat: Maintain caloric intake even with reduced appetite
- Sleep: Prioritize rest, avoid sleeping pills
Trekking pace tips:
- The "conversational pace" rule: you should be able to hold a conversation while walking
- Take rest steps on steep sections
- Match the slowest member's pace
- Avoid competitive attitudes about speed
Monitoring Tools
Pulse oximeter:
- Measures blood oxygen saturation (SpO2) and heart rate
- Useful for tracking trends, not absolute values
- Normal at altitude: 75-90% (varies by individual and altitude)
- Concerning: SpO2 dropping significantly from your baseline, especially combined with symptoms
- Not a substitute for symptom assessment
Symptom diary:
- Record Lake Louise scores daily
- Note any symptoms and their severity
- Track improvement or worsening trends
- Share with your guide
For guidance on tracking your blood oxygen, see our pulse oximeter and altitude monitoring guide.
Dehydration Warning Signs & Prevention
The 5 warning signs of dehydration are dark yellow urine (or passing very little), a dry mouth and intense thirst, headache and dizziness, unusual fatigue or muscle cramps, and a rapid heartbeat. To prevent dehydration while trekking in Nepal, drink 3-4 litres of water per day (4-5 litres on active days above 3,000m), add electrolytes, sip before you feel thirsty, and aim to keep your urine pale yellow to clear.
Dehydration deserves its own section because it is both common and dangerous at altitude. The Himalayan air is cold and bone-dry, you breathe faster and deeper (losing water with every exhalation), and the cold blunts your sense of thirst, so most trekkers under-drink without realising it. Worse, dehydration thickens your blood, slows acclimatization, and produces a headache and fatigue that are nearly identical to early AMS — making it harder to read your own body when it matters most.
The 5 Warning Signs of Dehydration
| # | Warning Sign | What to Look For |
|---|---|---|
| 1 | Dark or scant urine | Urine that is dark yellow, amber, or strong-smelling — or going hours without needing to urinate. The single most reliable field test. |
| 2 | Dry mouth and strong thirst | A sticky, dry mouth, cracked lips, and thirst that does not ease after a few sips. By the time you feel very thirsty you are already mildly dehydrated. |
| 3 | Headache and dizziness | A dull headache and light-headedness when you stand — easy to mistake for AMS, which is exactly why hydrating first is the standard first response. |
| 4 | Fatigue and muscle cramps | Disproportionate tiredness, heavy legs, and cramping calves or hands as fluid and electrolyte levels fall. |
| 5 | Rapid heartbeat and reduced sweating | A faster-than-normal resting pulse and noticeably less sweat even on a steep climb, as your body conserves fluid. |
Pro Tip
If you can only remember two warning signs of dehydration, remember these: dark urine and persistent thirst with a dry mouth. Both appear early, both are easy to check on the trail, and both respond quickly to drinking water with electrolytes.
How to Tell If You're Dehydrated on the Trail
You do not need equipment — three quick checks work at any tea house:
- The urine test: Pale yellow to clear is well hydrated; dark yellow or amber means drink now. This is the gold standard at altitude.
- The skin-pinch test: Pinch the skin on the back of your hand and release. If it snaps back instantly you are hydrated; if it stays "tented" for a second or two, you are dehydrated.
- The thirst-and-energy check: Strong thirst, a dry mouth, a nagging headache, and unusual fatigue together are a clear signal to stop and rehydrate before continuing.
Severe Dehydration Signs (Seek Help)
Severe dehydration is a medical concern in its own right and amplifies altitude illness. Treat the following as warning signs that need rest, aggressive rehydration with oral rehydration salts (ORS), and, if they do not improve, descent or medical attention:
- Little or no urine for 8+ hours, or very dark urine
- Sunken eyes, very dry skin, and no tears
- Confusion, irritability, or difficulty concentrating
- Rapid, weak pulse and rapid breathing
- Fainting, severe dizziness, or inability to keep fluids down (vomiting)
Dehydration vs. Altitude Sickness
Dehydration and AMS share headache, dizziness, nausea, and fatigue. The safe rule when trekking in Nepal: rehydrate first. Drink 500ml-1 litre of water with electrolytes, rest 30-60 minutes, and reassess. If symptoms ease, dehydration was likely the cause. If a headache or nausea persists despite good hydration, treat it as AMS — do not ascend, and follow the turnaround rules above.
How to Prevent Dehydration While Trekking
- Drink to a target, not to thirst: 3-4 litres daily minimum, 4-5 litres on active days above 3,000m. Start sipping before you feel thirsty.
- Add electrolytes: Plain water alone can dilute your sodium. Use ORS sachets, electrolyte tablets, or rehydration powders, especially on big climbs and pass days.
- Carry two 1-litre bottles and drink on a schedule (a few mouthfuls every 15-20 minutes) rather than gulping at breaks.
- Count hot drinks: Tea, soup, and the broth in dal bhat all add to your intake — tea houses make this easy.
- Purify safely: Treat tea-house and stream water rather than buying plastic bottles. See our water purification guide.
- Limit dehydrating habits: Avoid alcohol and minimise caffeine above 3,000m; both increase fluid loss. Note that Diamox is a diuretic, so trekkers taking it must drink even more.
- Check your urine daily: Pale yellow to clear is your goal. Waking once at night to urinate is a good sign you are well hydrated.
For a deeper plan, see our dedicated water purification and hydration guide and altitude nutrition strategy.
Medication Guide
Several medications can help prevent or treat altitude illness. Understanding their proper use, dosing, and limitations is essential.
Acetazolamide (Diamox)
Diamox is the most widely used and studied medication for altitude illness prevention. It works by acidifying the blood, which stimulates breathing and improves oxygenation during sleep.
How it works:
- Inhibits carbonic anhydrase enzyme
- Causes mild metabolic acidosis
- Stimulates respiratory drive
- Improves sleep quality at altitude
- Speeds acclimatization
Preventive use:
- Dose: 125-250mg twice daily
- Start: 1-2 days before ascending above 3,000m
- Continue: Until at highest point or beginning descent
- Effectiveness: Reduces AMS incidence by approximately 50%
Treatment use (for mild-moderate AMS):
- Dose: 250mg twice daily
- Continue: Until symptoms resolve and descent complete
- Combined with rest or descent
Diamox Does NOT Mask Symptoms
A common misconception is that Diamox hides altitude symptoms, preventing you from knowing you're sick. This is false. Diamox speeds your body's natural acclimatization process. You will still experience symptoms if you ascend too fast—Diamox doesn't eliminate the need for proper pacing. You'll know if you're getting AMS.
Side effects (common and expected):
- Tingling in fingers, toes, lips (paresthesia)—nearly universal
- Increased urination (diuretic effect)
- Altered taste, especially carbonated drinks taste flat
- Mild nausea (usually transient)
Contraindications:
- Sulfa drug allergy (Diamox is a sulfonamide)
- Severe kidney or liver disease
- Pregnancy
- History of severe reaction to acetazolamide
Important notes:
- Diamox is a prescription medication—obtain from your doctor before travel
- Available in Kathmandu pharmacies, but get it before you leave home
- Stay well hydrated (the diuretic effect can cause dehydration)
- Test the medication before your trip to check for allergy
Dexamethasone (Decadron)
Dexamethasone is a powerful steroid used for HACE treatment and sometimes HACE/severe AMS prevention in specific circumstances. It's not a first-line preventive medication.
How it works:
- Reduces brain swelling (cerebral edema)
- Decreases inflammation
- Provides rapid symptom relief in emergencies
Emergency treatment for HACE:
- Dose: 8mg initial, then 4mg every 6 hours
- Purpose: Buys time for descent
- Critical: Descent is still required—dexamethasone is not a cure
Emergency treatment for severe AMS:
- Dose: 4mg every 6 hours
- Combined with immediate descent
- Stop once at safe altitude
Why it's NOT for routine prevention:
- Powerful steroid with significant side effects
- Can mask symptoms, leading to dangerous decisions
- Withdrawal can cause rebound symptoms
- Reserved for emergencies
Side effects:
- Mood changes (euphoria, irritability)
- Insomnia
- Increased appetite
- Can mask symptoms (dangerous)
- With prolonged use: many serious effects
When to carry dexamethasone:
- Treks going above 5,000m with limited evacuation options
- Remote routes where descent may take days
- Should be carried by guide or designated group member
- Requires medical knowledge for proper use
Nifedipine (Procardia)
Nifedipine is a calcium channel blocker used specifically for HAPE prevention and treatment.
How it works:
- Dilates pulmonary blood vessels
- Reduces pulmonary artery pressure
- Decreases fluid accumulation in lungs
HAPE prevention (for those with history):
- Dose: 30mg extended-release twice daily
- Start: Day before ascent above 3,000m
- Continue: Until descent or 5 days at highest altitude
HAPE treatment:
- Dose: 30mg extended-release every 12 hours
- Combined with immediate descent
- Oxygen if available
Side effects:
- Headache
- Flushing
- Dizziness
- Low blood pressure
- Rapid heart rate
Important notes:
- Prescription required
- Only for HAPE, not AMS or HACE
- Usually only prescribed for those with previous HAPE
- Descent remains essential treatment
Medications to AVOID at Altitude
Sleeping pills (benzodiazepines, zolpidem, etc.):
- Depress breathing
- Dangerous with low oxygen
- Can mask HACE symptoms
Narcotic pain medications:
- Depress breathing
- Mask symptoms
- Impair judgment
Alcohol:
- Depresses breathing
- Causes dehydration
- Impairs judgment
- Masks symptoms
Medication Summary Table
| Medication | Primary Use | Typical Dose | When to Use | Prescription Required |
|---|---|---|---|---|
| Acetazolamide (Diamox) | AMS prevention & treatment | 125-250mg 2x daily | Start 1-2 days before high altitude | Yes |
| Dexamethasone | HACE emergency treatment | 8mg, then 4mg every 6 hours | HACE symptoms, severe AMS | Yes |
| Nifedipine | HAPE prevention & treatment | 30mg ER 2x daily | HAPE history or symptoms | Yes |
| Ibuprofen | AMS headache relief | 400-600mg as needed | Mild headache | No |
| Paracetamol | AMS headache relief | 500-1000mg as needed | Mild headache | No |
Treatment Protocols
When altitude illness occurs despite prevention efforts, proper treatment can prevent progression and save lives. These protocols are based on Wilderness Medical Society guidelines.
Mild AMS Treatment Protocol
Recognition: Headache plus at least one other symptom (Lake Louise Score 3-5)
Treatment steps:
- Stop ascending—do not gain any sleeping altitude
- Rest at current altitude
- Hydrate aggressively (3-4 liters/day)
- Treat symptoms:
- Ibuprofen or paracetamol for headache
- Light, carbohydrate-rich meals
- Avoid alcohol
- Consider Diamox 250mg twice daily if not already taking
- Monitor symptoms using Lake Louise scoring every 6-12 hours
- Descend if symptoms worsen or don't improve in 24-48 hours
Expected outcome: Most mild AMS resolves within 24-48 hours with rest at same altitude. Once symptoms are completely gone for 24 hours, careful ascent can resume.
Moderate AMS Treatment Protocol
Recognition: Lake Louise Score 6+, multiple significant symptoms, or mild AMS not improving after 24-48 hours
Treatment steps:
- Descend 500-1,000m
- Start Diamox 250mg twice daily if not already taking
- Rest at lower altitude
- Hydrate aggressively
- Treat symptoms with ibuprofen/paracetamol
- Monitor closely for any HACE signs
- Consider evacuation if symptoms don't improve with descent
Expected outcome: Symptoms should improve within hours of descent. Complete resolution may take 1-3 days. Re-ascent only after full recovery and should be slower.
HACE Emergency Treatment Protocol
Recognition: Ataxia, confusion, severe unrelenting headache, altered mental status
HACE Treatment: Time Critical
HACE is a medical emergency. Treatment must begin immediately. Every hour of delay increases mortality risk.
Immediate actions:
- DESCEND IMMEDIATELY—this is the priority
- Descend as far as possible, minimum 500-1,000m
- Descend at night if necessary
- Evacuate by helicopter if available
- Administer dexamethasone (if available):
- 8mg immediately (oral, IM, or IV)
- Then 4mg every 6 hours
- Administer oxygen if available:
- High flow (4-6 liters/minute)
- Use Gamow bag/portable altitude chamber if available and descent impossible
- Do NOT allow patient to walk alone—they are disoriented
- Call for evacuation if descent is impossible or too slow
Critical points:
- Dexamethasone is not a substitute for descent—it buys time
- Continue descent even if patient improves with medication
- Patient may resist descent due to confusion—insist firmly
- Evacuation to medical facility for monitoring after stabilization
HAPE Emergency Treatment Protocol
Recognition: Breathlessness at rest, cough with bloody/frothy sputum, severe fatigue, chest congestion, blue lips
HAPE Treatment: Minutes Matter
HAPE can kill within 12 hours. This is the deadliest form of altitude illness. Treatment must begin immediately.
Immediate actions:
- DESCEND IMMEDIATELY—even more critical than in HACE
- Descend as far as possible, minimum 1,000m
- Minimize patient's physical exertion (evacuation by others, animal, or helicopter)
- Descend at night if necessary
- Administer oxygen (highest priority after descent):
- High flow (4-6 liters/minute) if available
- Even low-flow oxygen helps
- Administer nifedipine (if available):
- 30mg extended-release immediately
- Repeat every 12 hours
- Use Gamow bag if available and descent impossible
- Keep patient warm—hypothermia worsens HAPE
- Call for helicopter evacuation immediately
Critical points:
- HAPE patients should NOT walk if possible—exertion worsens the condition
- Descent improves symptoms rapidly (often within hours)
- Even partial descent (300-500m) can be life-saving
- Oxygen is extremely valuable—prioritize its use for HAPE
- Continued monitoring required even after improvement
Gamow Bag / Portable Altitude Chamber
The Gamow bag is a portable hyperbaric chamber that simulates descent by increasing air pressure inside the bag. It's a life-saving device when descent is impossible.
How it works:
- Patient lies inside sealed bag
- Manual pump increases pressure (equivalent to 1,500-3,000m descent)
- Provides emergency treatment while evacuation is arranged
Availability in Nepal:
- Himalayan Rescue Association posts (Pheriche, Manang)
- Some high-altitude lodges
- Some trekking agency guides carry them
- Rarely carried by individual trekkers
Limitations:
- Does not replace descent
- Patient cannot eat, drink, or urinate inside
- Someone must continuously pump to maintain pressure
- Temporary measure only
Trek-Specific Altitude Considerations
Different Nepal trekking routes present different altitude challenges. Understanding the specific profile of your planned route helps you prepare appropriately.
Everest Base Camp Trek
Route profile: Gradual ascent from Lukla (2,860m) to Gorak Shep (5,164m) and EBC (5,364m)
Critical altitude points:
| Location | Altitude | Significance |
|---|---|---|
| Namche Bazaar | 3,440m | First major altitude gain, mandatory rest day |
| Tengboche | 3,870m | First night above 3,500m |
| Dingboche | 4,410m | Entering high-risk zone, mandatory rest day |
| Lobuche | 4,940m | Very high altitude, common AMS symptoms |
| Gorak Shep | 5,164m | Highest sleeping point, maximum stress |
| EBC | 5,364m | Day visit only, not sleeping altitude |
| Kala Patthar | 5,545m | Optional highest point, pre-dawn climb |
Key danger zones:
- Namche to Tengboche: First significant multi-day high altitude exposure
- Dingboche to Lobuche: Crossing into very high altitude zone
- Lobuche to Gorak Shep: Final push, cumulative fatigue, highest sleeping altitude
Recommended acclimatization:
- Rest day at Namche (day 4)
- Rest day at Dingboche (day 7)
- Consider extra day if any symptoms
For complete route details, see Everest Base Camp Trek Guide.
Everest Three Passes Trek
Route profile: Extended high-altitude circuit crossing three 5,000m+ passes
Critical altitude points:
| Pass/Location | Altitude | Challenge |
|---|---|---|
| Kongma La | 5,535m | Technical terrain, steep approach |
| Cho La | 5,420m | Glacier crossing, requires good weather |
| Renjo La | 5,360m | Exposed, weather-dependent |
| Gokyo Ri | 5,357m | Optional but spectacular sunrise hike |
| Kala Patthar | 5,545m | Highest point, often combined with EBC |
Key danger zones:
- All three passes involve sustained time above 5,000m
- Multiple consecutive days at extreme altitude
- Weather delays can extend high-altitude exposure
- Technical terrain combined with altitude stress
Recommended acclimatization:
- All standard EBC acclimatization days
- Additional day before each pass if any symptoms
- Minimum 18-20 day itinerary
- This route is NOT for first-time high-altitude trekkers
For complete route details, see Everest Three Passes Trek Guide.
Annapurna Circuit
Route profile: Long circuit with gradual ascent to Thorong La (5,416m)
Critical altitude points:
| Location | Altitude | Significance |
|---|---|---|
| Manang | 3,540m | Major acclimatization hub |
| Thorong Phedi | 4,450m | Pre-pass camp |
| High Camp | 4,925m | Optional higher sleeping point |
| Thorong La | 5,416m | Highest point—early morning crossing |
| Muktinath | 3,800m | Post-pass descent destination |
Key danger zones:
- Thorong Phedi to Thorong La: Single-day 1,000m gain, starts at night
- Thorong La crossing: Extended time above 5,000m, weather exposure
- Rapid descent risk: Temptation to rush given schedule pressures
Recommended acclimatization:
- Rest day in Manang
- Optional day hike to Ice Lake (4,600m) from Manang
- Consider sleeping at High Camp for gradual gain
- Start pass crossing very early (3-4 AM) to reach Muktinath same day
For complete route details, see Annapurna Circuit Trek Guide.
Annapurna Base Camp
Route profile: Moderate altitude with relatively quick ascent to 4,130m
Critical altitude points:
| Location | Altitude | Significance |
|---|---|---|
| Deurali | 3,230m | Last village before base camp |
| Machapuchare BC | 3,700m | Common overnight stop |
| Annapurna BC | 4,130m | Highest point |
Key considerations:
- Lower maximum altitude than EBC (4,130m vs 5,364m)
- Faster ascent rate in some itineraries
- Less time for acclimatization
- AMS still possible and common
- Often perceived as "easier" leading to inadequate preparation
Recommended approach:
- Minimum 7-day itinerary (10+ is better)
- Don't rush to ABC in one push from lower camps
- Consider overnight at MBC before ABC
- Hydrate aggressively
For complete route details, see Annapurna Base Camp Trek Guide.
Manaslu Circuit
Route profile: Remote circuit with Larkya La pass crossing at 5,160m
Critical altitude points:
| Location | Altitude | Significance |
|---|---|---|
| Samagaon | 3,530m | Main acclimatization village |
| Samdo | 3,875m | Pre-pass village |
| Dharamsala | 4,460m | Night before pass |
| Larkya La | 5,160m | Highest point, challenging crossing |
Key danger zones:
- Dharamsala to Larkya La: 700m gain to pass, long day
- Limited evacuation options: Remote route, helicopter access challenging
- Weather dependence: Pass can close unexpectedly
Recommended acclimatization:
- Rest day in Samagaon
- Day hike above Samdo
- Minimum 14-day itinerary
For complete route details, see Manaslu Circuit Trek Guide.
Langtang Valley
Route profile: Moderate altitude, good acclimatization trek
Critical altitude points:
| Location | Altitude | Significance |
|---|---|---|
| Langtang Village | 3,430m | Rebuilt after 2015 earthquake |
| Kyanjin Gompa | 3,870m | Trek destination |
| Tserko Ri | 4,984m | Optional day hike |
Why Langtang is good for acclimatization:
- Maximum sleeping altitude 3,870m (manageable for most)
- Gradual ascent from Kathmandu
- Day hikes to higher points available
- Good preparation for higher routes
For complete route details, see Langtang Valley Trek Guide.
Emergency Evacuation
When altitude illness becomes severe, evacuation may be life-saving. Understanding how evacuation works in Nepal helps you prepare and respond effectively.
Helicopter Rescue in Nepal
How it works:
- Helicopters can reach most major trekking areas
- Response time: 2-6 hours depending on location and weather
- Operated by private companies (Simrik Air, Altitude Air, Fishtail Air, others)
- Pilots are experienced in high-altitude rescue
Requesting evacuation:
- Your guide contacts the agency or rescue coordinator
- Agency contacts helicopter company
- Insurance verification (critical step)
- Helicopter dispatched when weather permits
- Landing zone identified (flat area, marked if possible)
Limitations:
- Weather can ground helicopters for hours or days
- Maximum operating altitude approximately 6,000m
- Some areas have no landing zones
- Night flying extremely limited
- Costs $3,000-5,000+ USD without insurance
Insurance Requirements
Insurance Is Non-Negotiable
Helicopter evacuation without insurance can bankrupt you. A single rescue can cost $5,000-8,000 USD or more. Verify your insurance covers:
- Helicopter evacuation
- Evacuation from your maximum planned altitude (6,000m+ recommended)
- Medical treatment abroad
- Repatriation
- Trip cancellation
Do not assume standard travel insurance is adequate. Most basic policies cap altitude coverage at 3,000-4,000m.
Recommended insurance coverage:
- Evacuation coverage to minimum 6,000m altitude
- Medical coverage minimum $100,000 USD
- Explicit helicopter evacuation coverage
- 24/7 emergency contact number
Reputable insurers for high-altitude trekking:
- World Nomads (verify altitude coverage)
- Global Rescue
- IMG (International Medical Group)
- Specialty mountaineering insurers
Emergency Communication
Your guide should have:
- Satellite phone or InReach device
- Emergency contact numbers
- Knowledge of helicopter landing zones
- Relationship with evacuation coordinators
Emergency numbers in Nepal:
- Nepal Police: 100
- Tourist Police: 1144
- Himalayan Rescue Association (Kathmandu): +977-1-4440292
- CIWEC Clinic (Kathmandu): +977-1-4424111
Himalayan Rescue Association (Pheriche)
High-altitude medical post in Everest region
HRA Clinic Manang
High-altitude medical post in Annapurna region
CIWEC Clinic Kathmandu
Western-standard travel medicine clinic
Nepal Tourist Police
24/7 emergency line for tourists
Nepal Police Emergency
General emergency services
Helicopter evacuation cost: $3,000-5,000+ USD (must be covered by travel insurance)
Standard travel insurance often excludes high-altitude trekking. Verify your policy explicitly covers helicopter evacuation to at least 6,000m altitude before departing.
When Evacuation Isn't Possible
Sometimes weather, location, or other factors make helicopter evacuation impossible. In these situations:
Ground evacuation options:
- Descent by foot (patient walking with support)
- Descent by horse or yak (available in some areas)
- Stretcher carry by porters (exhausting, slow, last resort)
Stabilization while waiting:
- Continue treatment protocols (descent, medications, oxygen)
- Use Gamow bag if available
- Keep patient warm and hydrated
- Monitor vital signs and symptoms
- Prepare for extended management
Critical principle: Even when evacuation is delayed, continued descent by any means improves outcomes. Never wait passively hoping for helicopter rescue.
Frequently Asked Questions
Key Takeaways
Understanding altitude sickness could save your life—or the life of a fellow trekker. Here's what matters most:
Prevention is everything:
- Follow the golden rules: gradual ascent (300-500m/day), mandatory rest days, climb high/sleep low
- Hydrate aggressively (3-4+ liters/day)
- Never ascend with symptoms
- Consider prophylactic Diamox if appropriate
Recognition saves lives:
- Know the symptoms of AMS, HACE, and HAPE
- Monitor yourself and fellow trekkers daily
- The ataxia test (heel-to-toe walking) is your HACE early warning system
- Breathlessness at rest is a HAPE emergency
Action is non-negotiable:
- Stop ascending at the first sign of symptoms
- Descend if symptoms worsen or don't improve
- Descend immediately for any HACE or HAPE signs
- "When in doubt, go down" is your mantra
Preparation matters:
- Choose appropriate itineraries with adequate acclimatization time
- Ensure proper insurance covering high-altitude evacuation
- Carry or have access to emergency medications
- Know the emergency contacts and evacuation procedures
The Himalaya offer some of the world's most spectacular trekking experiences. With proper knowledge, appropriate planning, and the wisdom to listen to your body, you can enjoy these mountains safely. The key is respect—respect for altitude, respect for symptoms, and respect for the simple truth that descent is always an option, and sometimes it's the only right choice.
⚠️ Helicopter Rescue Scam Warning: Nepal has seen documented cases of fraud where some guides exaggerate altitude sickness symptoms and inflate helicopter and hospital bills submitted to insurers. Always use reputable agencies, contact your insurance provider before evacuation when possible, and trust your own judgment about your condition.
Related Resources
Route Guides
- Everest Base Camp Trek Complete Guide
- Everest Three Passes Trek Guide
- Annapurna Circuit Trek Guide
- Annapurna Base Camp Trek Guide
- Manaslu Circuit Trek Guide
- Langtang Valley Trek Guide
- Gokyo Lakes Trek Guide
Planning Resources
- Nepal Trekking Permits Explained
- Best Time to Trek Everest Region
- Water Purification & Hydration Guide
- Pulse Oximeter & Altitude Monitoring
- Hidden Costs on Nepal Treks
Region Guides
- Everest-Khumbu Region Overview
- Annapurna Region Overview
- Langtang Region Overview
- Manaslu Region Overview
Safety & Altitude Resources
- Altitude Sickness Prevention & Treatment
- Acclimatization Guide for Nepal Trekking
- Diamox for Altitude Sickness
- HAPE & HACE Emergency Guide
- Altitude Nutrition & Eating Strategy
Choosing an Agency
- How We Verify Trekking Agencies
- Safety-Ready Badge Standards
- Compare Everest Base Camp Agencies
- Compare Annapurna Circuit Agencies
This guide is based on current guidelines from the Wilderness Medical Society, International Society for Mountain Medicine, and Himalayan Rescue Association. While we strive for accuracy, this information is for educational purposes and does not replace professional medical advice. Consult with a healthcare provider before undertaking high-altitude trekking, especially if you have pre-existing medical conditions.
Last updated: June 2026. For corrections or updates, contact our editorial team.